by admin | Nov 12, 2017 | Blog, Cardiac Devices, Latest ISfTeH News:, Recent Articles
• « Business models for medical apps » presented by Ruben Casado Arroyo (chaired by @enricogaiani and @brittaboeckmann).
• « Issues for telemedecine in 2017 » (presented by Francesco Petracca): data privacy, financial reinbursement, regulation and medical responsibility, app testing. What’s your opinion?
• Raf van Goethem, lawyer from Bergium, lectured on the « Legal framework for the use of telemedical care in Europe » in a session chaired by Frank Lievens and myself. Hi teached us how vulnerable doctors are when trying to treat patients by telemedecine, due to regulatory flaws in the EU legislation. Also, before deploying a telemedicine project or being involved in one, check the applicable rules and legislation, check the obligations for each actor (who is responsible for what), make contractual arrangements, and check the insurance policy (is telemedicine included?)…
• The « Young investigator award » session was chaired by Paul Dendale, Enrico Caiani and Nico Bruining. Impressive presentations of each participant.
Overall, an excellent opportunity to learn and socialize with fellows colleagues.








 • « Business models for medical apps » presented by Ruben Casado Arroyo (chaired by @enricogaiani and @brittaboeckmann).
• « Business models for medical apps » presented by Ruben Casado Arroyo (chaired by @enricogaiani and @brittaboeckmann).
• « Issues for telemedecine in 2017 » (presented by Francesco Petracca): data privacy, financial reinbursement, regulation and medical responsibility, app testing. What’s your opinion?
• Raf van Goethem, lawyer from Bergium, lectured on the « Legal framework for the use of telemedical care in Europe » in a session chaired by Frank Lievens and myself. Hi teached us how vulnerable doctors are when trying to treat patients by telemedecine, due to regulatory flaws in the EU legislation. Also, before deploying a telemedicine project or being involved in one, check the applicable rules and legislation, check the obligations for each actor (who is responsible for what), make contractual arrangements, and check the insurance policy (is telemedicine included?)…
• The « Young investigator award » session was chaired by Paul Dendale, Enrico Caiani and Nico Bruining. Impressive presentations of each participant.
Overall, an excellent opportunity to learn and socialize with fellows colleagues.

by admin | Nov 12, 2017 | Blog, Latest ISfTeH News:, Recent Articles
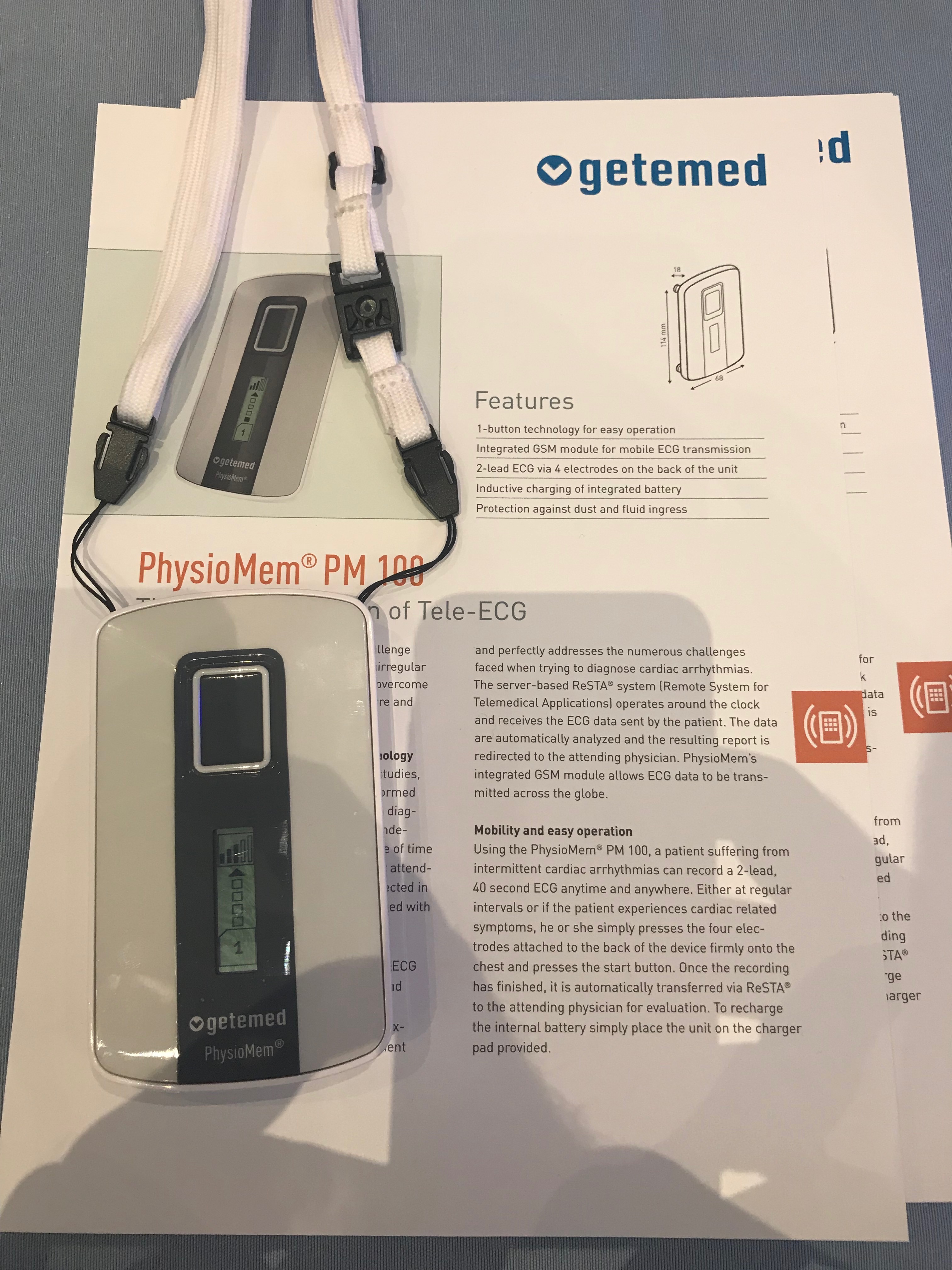
I had the pleasure to be invited as faculty to the 4th European Congress on eCardiology and eHealth, in Berlin, 8-10 november 2017. I will try to resume in the following 3 posts what impressed me the most concerning the lectures, devices and posters.
So concerning the lectures, below are the ones that attracted my attention. I further invite you to consult the #ecardio2017 website for the full presentations (plus take a look at the photos attached):
• The inaugural session talked about advances in mobile health, and was chaired by Enrico Caiani and Hugo Saner. Enriching and inspiring session.
• « Business models and solutions » session, chaired by Paul Dendale and Ines Frederix: Teleconsultation works, concluded Mr. Huyghe from Philips.
• « Instant messaging and selfies: the future of telemedicine ? » by prof. M.Mars: whatsapp and selfies use for medical purpose is very usual but raises ethical concerns regarding patient consent and private data. Would you use it in your daily practice?
• « Virtual cardiac emergency unit: the use of mobile technologies in acute cardiology » presented by E. De Kluiver:« don’t come to us, we come to you » (patients are seen by specialized nurses and treatment is conducted by hospital cardiologist: diuretics, inotropes).








by admin | Jul 24, 2017 | Blog, Patient information
According to an English study, 16% of the victims had been hospitalized in the previous month for atypical symptoms.
In England, one in six fatal myocardial infarction patients were hospitalized in the month before the diagnosis of infarction was reported by doctors. Could the fatal accident have been avoided? This is the question raised by the study conducted by Professor Perviz Asaria and his colleagues at Imperial College in London, together with researchers from Harvard, USA. The results were published in The Lancet Public Health. The researchers studied the medical record of the 135950 people aged 35 and over who died of a myocardial infarction in England between 2006 and 2010. They found that half had already been hospitalized in the four weeks before the accident Fatal, or a group of 66490 patients.
Missed opportunities or classification errors
They then dismissed two-thirds of those diagnosed with myocardial infarction, either directly or secondarily, and concentrated on the 21677 patients who were not thought of. For the most part (59%), the reasons for hospitalization did not particularly favor a cardiac problem (pneumonia, cancer, infection, fracture of the femur neck, etc.). But for 7566 patients (35%), the diagnosis made during the hospitalization was that of another cardiac disorder, including heart failure or rhythm disorder (atrial fibrillation in particular). In 1368 patients (6%), there were also symptoms suggestive of myocardial infarction, such as shortness of breath or atypical chest pain.
The fact that symptoms are underestimated does not mean that it is a automatically a medical error, but the study shows that the medical profession needs to improve risk stratification to better detect who is at risk of dying from an infarction in the event of atypical symptoms.
Establishing a prognosis is always more difficult than making a diagnosis a posteriori, and there is no question of keeping in the hospital all the people complaining of a gastric embarrassment
As for the chest pain typical of the infarction, a study conducted in North Carolina between 1994 and 2006 showed that it was absent in two thirds of infarcts. Doctors are very good at treating heart attacks when they are the primary cause of admission to the hospital, but much less when they are comorbid (pathology associated with another diagnosis, or when it comes to identifying subtle symptoms that could lead to the imminence of a myocardial infarction.
Failure in detection
These results should encourage physicians to be more vigilant, reduce the risk of missing these symptoms and ultimately save lives.
In France, it is estimated that 120000 infarcts (or acute coronary syndrome) occur each year. Improvements in the management of patients with chest pain have significantly reduced myocardial infarction mortality. But margins of progress still exist, as one-third of patients lose time by visiting their family doctor or by going to their own emergencies instead of directly calling the 112 or 15 emergency service, when they experience typical symptoms infarction (ongoing chest pain).

by admin | Jul 24, 2017 | Blog, Patient information
The chances of long-term survival increase significantly with prompt intervention following a cardiac arrest.
Every year in France, 40,000 people suffer from cardiac arrest. In Paris the chances of survival at 30 days were close to 10% in 2016, compared with 6% five years earlier. In Denmark, a country with 5.6 million inhabitants, the national registry’s rate of survival was 12% in 2013, compared to 5% in 2001. In the meantime, training of general population in resuscitation gestures and protocols in order to restart the heart was performed (cardiac massage started by a witness immediately after calling a specialized team, defibrillation if necessary). The result was a rise of the efficacy of resuscitation maneuvers from 18% in 2001 to 60% in 2013, according to the study published in the European Heart Journal. A key factor in increasing the survival of victims, survival which increased by 10%. It is important to note that the increase in resuscitation gestures by controls is not the only reason for this improvement. Quality care provided by emergency services and hospital care add to these results.
Since 2013, there has been a consensus within the Danish Cardiovascular Society that all victims of cardiac arrest whose heart is restarted (“recovered cardiac arrest”, in medical jargon) should benefit rapidly from a coronary angiography (examination to visualize the heart’s arteries), and, if one of them is occluded, a gesture to restore blood flow (angioplasty with stent). This means that they are brought by the emergency services directly to a hospital with a technical interventional cardiology platform.
By taking the 41,000 cardiac arrests collected in the Danish register between 2001 and 2013, Dr. Tranberg and his colleagues observed that 16000 patients had died before arriving to a hospital, 18000 were sent to local hospitals and 7000 were taken to an interventional cardiology center. The rate of survival was 29%. However, the study shows that the remoteness of the center does not significantly influence the survival rate. Once cardiac arrest is recovered, you can afford to lose a little time to go to a particularly experienced cardiac center.
In France, the transfer to a center with an interventional cardiology unit has already been carried out almost systematically for several years, but the quality of the hospital’s resuscitation service must also be taken into account, because the in-hospital management is almost as important as the initial phase of the recovery.
Regardless of the quality of medical services of the hospital where a cardiac arrest victim are transferred, the first few minutes are crucial. All adults should have the basic notions how to perform cardiac massage. Even before the transfer to a hospital, the most important thing is the initial management: the duration of the cardiac arrest before the first massage and the time taken to recover an effective cardiac rhythm.

by admin | Jul 20, 2017 | Blog, Patient information
High blood pressure, how to treat it, what hypertension means and how it affects us are questions that can be found in varied variants of answers, but the medical correctness of these types of questions can be found in this post.
Blood pressure represents physics laws as any fluid inside a container and exerts pressure on its walls. The fluid we are talking about is the blood that is in permanent circulation in the blood vessels and is constantly exerting tension on them.
The tension we are talking about is blood pressure (BP), which is the pressure exerted inside the blood vessels. Blood circulation has two values due to myocardial contraction and relaxation, therefore blood pressure is expressed in two sets of values: one higher (systolic) and a smaller one (diastolic).
Blood pressure is measured in mm / hg, meaning millimeter mercury column, and the abbreviated form is to divide the values at 10, so the correct expression is like an example of 120/80 mm / Hg while the abbreviated form is 12/8.
Normal range.
Blood pressure values can not be categorized into a clear figure, but rather within an interval because blood pressure varies as normal limits depending on:
– Weight: A person under 55 kg has a value of 10 mm / Hg at lower acceptable limits, while a person with a value between 55-85 is exactly the average of the values, and between 85-110 is accepted by 10 Mm / Hg above the admitted limit, as in people over 110 kg most likely will be a obesity hypertension, that is to say even at a value of 20-30 mm / Hg but which is not necessarily accepted; some expect increased value in these people with obesity;
– Age: For young adults aged 16-25, the tension may be either exactly the normal range or exactly 10 units below this average. For the mature adult: 25-45 years of age should fit exactly within the medium range. While between 45 and 60 years, this value is even 10 units over this range, and over 60 years there may be hypertension or hypotension (so-called physiological), that is, 10, even 20 units above the mean .
– Physical Conformity: If a physical person is athletic conformation or practicing regular sports, or has practiced a performance sport for more than 10 years and has not passed more than 10 years since the end of performance sports, a Adaptability of the heart (as a rhythm) a decrease in this rhythm and respiratory rate as well as blood pressure, so it is possible for these people to have a value of less than 10 in the category of the person.
– In these characteristics where small varieties can be accepted, there can be added also environmental and environmental conditions: smoking, alcohol consumption. Psychosocial factors can also be added: stress, psychic shock recently. At the same time, a physical exercise may have to be considered that may have been given up before the voltage measurement (less than 5 minutes before blood pressure measurement).
A correct measurement to confirm the certainty of possible blood pressure pathologies should include three consecutive measurements at a distance of 3-5 minutes apart, alternating the two arms.
Hypotension and Hypertension – Values, Explanations, Symptoms
For clarification, an average value for a young adult or mature adult is 90-139 mm / Hg of systolic and 60-89 of diastolic pressure.
Pathology (Sistolic/ Diastolic)
Hypotension: <90 <60
Physiological tension: 90-139/60-89
Hypertension first class: 140-159/90-99
Hypertension second class: 160-180/100-110
Hypertension.third class:> 180/> 110
Hypotension is the condition of blood pressure below normal values, i.e. below a systolic value of 90 and an adjacent one, diastolic below 60 mm / Hg. If this tension is in the range of -10 mmHg to both systolic and diastolic, and the person concerned is either a female patient with a body weight of 40-45 kg (or in some cases even more If the person is athletic performance or if the person’s fluid consumption is very low, there are already possible explanations for the hypotension.
A liquid consumption of less than 1 liter per day (although physiological consumption is 2-2.5 liters of fluid per day than those in food or other forms of liquids rather than water), is sufficient to favorize hypotension. Blood pressure is directly proportional to the circulating blood volume (a smaller amount of blood will exert a lower pressure on the walls).
Symptoms related to hypotension are: fainting, dizziness, feeling of choking that can be associated with a headache, dyspepsia (indigestion) or dysuria (painfur urination), and can progress to the loss of consciousness .
High blood pressure first class means an increase over the value of 140/90 of blood pressure and that can explain a heart failure at the onset of pathology, especially if the systolic value is 140 and the diastolic is 95-100. But in time, it has two paths, or it will be adapted by the body that will be able to compensate it, ie to adapt to these values, or it will evolve to grade 2 hypertension. A grade one hypertension will give in extremely rare cases complications that are generally referred to as hypertension, but progressive progression through second degree will later give these complications. Symptoms of the first degree hypertension include palpitations (which may also indicate associated cardiac dysfunction), a headache, or vertigo and pressure in the ears or in the eyelid.
Second-degree hypertension is already an important hypertension that needs to be treated and that already reveals some dysfunctions: cardiac, renal, or circulatory. This hypertension can cause complications such as: aneurysm (aortic or abdominal artery aneurysm), heart failure, chronic kidney pathologies, cardiac arrest or infarction as well as peripheral arterial pathology as well as coronary artery disease. Symptoms include tinnitus (headache), headaches (especially frontal), vertigo and dizziness as well as episodes of fainting.
Third-degree hypertension is a medical emergency, meaning a major dysfunction. Acute complications include stroke, heart attack, heart failure. hronic complications include: heart failure, coronary artery disease or thoracic/abdominal artery aneurysm.
Causes
Causes of hypertension originate from a combination of interactions between several factors, most of which are factors that have been acquired (living and environmental conditions also):
– Smoking and alcohol consumption: Although it acts by two different mechanisms, smoking causes both a respiratory and endothelial dysfunction that will also cause hypoxia and a deficient oxygen fixation on hemoglobin. However, alcohol will act through portal hypertension (portal system of the liver) and the portal hypertension will cause hypertension.
– Obesity: Obesity will form plaque atherosclerosis in the blood vessels and which in turn will aggravate blood circulation through the vessels. This will result in high blood pressure.
– Stress: In addition to a series of strict cardiac and cardiovascular pathologies other than hypertension, and an aggravating cause in ulcerative pathology, stress is a major incriminating factor in hypertension as well.
The main two organs that can favorize hypertension are the heart and the kidneys.
Pathologic vessels, i.e. weakening of vessel elasticity caused by deposition of atheromatous plaques, a decrease in elasticity due to age, or even clot formation can cause hypertension.